Written by: Amy Wagner, MEd, CHA, CPC, ICDCT-CM
More...
Posted 6/10/2020
As an experienced coder yourself, it is important to know how to present information to your staff and co-workers. Given the complexity of ICD-10, as well as the annual updates to the diagnosis data sets, there is always something new to learn and important skills to update and refresh. What are the best approaches to take as a trainer when the people in your audience are already experienced coders?
Why is Training Important? It is an OIG Expectation and Requirement!
Some may attend out of curiosity, but most people in your audience are there because it is a mandated training requirement of your organization. Make sure everyone signs in for “proof of presence” and offer a quiz or other type of evidence that the employee successfully completed the training. The Office of Inspector General (OIG) publishes “Compliance Guidance” documents for various types of health care providers. In each guidance, government expectations for training and education are stated. Excerpts from two OIG Compliance Guidance publications are provided below, one for a physician practice and one for a hospital.
Physician Practice Guidance
Step Four: Conducting Appropriate Training and Education
There are three basic steps for setting up educational objectives:
- Determining who needs training (both in coding and billing and in compliance);
- Determining the type of training that best suits the practice’s needs (e.g., seminars, in-service training, self-study or other programs); and
- Determining when and how often education is needed and how much each person should receive.
Coding and billing training on the Federal health care program requirements may be necessary for certain members of the physician practice staff or health care organization, depending on their respective responsibilities.
Some issues recommended by the OIG that could be covered in coding and billing training include:
- Coding requirements;
- Claim development and submission processes;
- Signing a form for a physician without the physician’s authorization;
- Proper documentation of services rendered;
- Proper billing standards and procedures and submission of accurate bills for services or items rendered to Federal health care program beneficiaries; and
- The legal sanctions for submitting deliberately false or reckless billings.
There is no set formula for determining how often training sessions should occur. The OIG recommends that there be at least an annual training program for all individuals involved in coding and billing aspects of the organization. Ideally, new billing and coding employees will be trained as soon as possible after assuming their duties and will work under an experienced employee until their training has been completed.
Hospital Guidance
The OIG dedicates a section to Claim Development and Submission Process compliance:
Policies and Procedures should:
- Provide for proper and timely documentation required of all physician and other professional services prior to billing to ensure that only accurate and properly documented services are billed;
- Emphasize that claims should be submitted only when appropriate documentation supports the claims and only when such documentation is maintained and available for audit and review;
- State that, consistent with appropriate guidance from medical staff, physician and hospital records and medical notes used as a basis for a claim submission should be appropriately organized and in a legible form for possible audit and review;
- Indicate that the diagnosis and procedures reported on the reimbursement claim should be based on the medical record and other documentation, and that the documentation necessary for accurate code assignment should be available to coding staff; and
- Provide that the compensation for billing department coders and billing consultants should not provide any financial incentive to improperly upcode claims.
Hospital Guidance on Conducting Effective Training and Education – The OIG indicates the following compliance training points to keep in mind:
- A variety of teaching methods, such as interactive training, and training in several different languages, particularly where a hospital has a culturally diverse staff, should be implemented.
- The OIG recommends that attendance and participation in training programs be made a condition of continued employment and that failure to comply with training requirements should result in disciplinary action, including possible termination, when such failure is serious.
- The hospital should retain adequate records of its training of employees, including attendance logs and material distributed at training sessions.
Always Start by Reviewing the Official Coding Guidelines Updated Each Year
The Centers for Medicare and Medicaid Services (CMS) posts the next fiscal year (FY) data files electronically in May, June or July each year. It is highly recommended that ICD-10-CM trainers download the electronic files (e-files) and review critical updates in the Guidelines, Index and Tabular. Then, prepare training information to review with your coders based on the updates affecting your specialty, department or facility type.
Remind coders that the Official Coding Guidelines do not take precedence over guidelines found in the Tabular. The Tabular must be referenced to be sure codes are not truncated and to guide you with additional directives for appropriate code assignment and sequencing. Review areas where common ICD-10-CM coding errors are made. See some of those areas below.
Combination Codes
A combination code is a single code used to classify two diagnoses, a diagnosis with an associated secondary process (manifestation), or a diagnosis with an associated complication. Combination codes are identified by referring to subterm entries in the Alphabetic Index and by reading the inclusion and exclusion notes in the Tabular.
Since the implementation of ICD-10-CM on October 1, 2015, sufficient time has elapsed that common errors being made in code selection can be identified. One of these is the lack of using proper combination codes. Many providers continue to report two codes when ICD-10-CM provides a single combination code. Diabetes coding is a great example.
When a patient with diabetes mellitus and polyneuropathy is treated, two codes should NOT be reported! Utilize ICD-10-CM guidelines to see both conditions are reported in one code.
Coding Error [applying old ICD-9 principle] | Correct Coding [utilizing features of ICD-10] |
E11.9 Type 2 diabetes mellitus without complications G62.9 Polyneuropathy, unspecified | E11.42 Type 2 diabetes mellitus with diabetic polyneuropathy; Type 2 diabetes mellitus with diabetic neuralgia |
Assign only the combination code when that code fully identifies the diagnostic conditions involved or when the Alphabetic Index directs.
Multiple codes should not be used when the classification provides a combination code that clearly identifies all of the elements documented in the diagnosis. When the combination code lacks necessary specificity in describing the manifestation or complication, an additional code should be used as a secondary code.
Etiology/Manifestation Conventions
ICD-10-CM does have an etiology/manifestation coding convention. Certain conditions have both an underlying etiology and multiple body system manifestations due to the underlying etiology. For such conditions, ICD-10-CM has a coding convention that requires the underlying condition be sequenced first and be followed by the manifestation. Wherever such a combination exists, there is a “use additional code” note at the etiology code, and a “code first” note at the manifestation code.
These instructional notes indicate the proper sequencing order of the codes, etiology followed by manifestation. In most cases, the manifestation codes will have in the code title “in diseases classified elsewhere.” Codes with this title are a component of the etiology/manifestation convention. The code title indicates that it is a manifestation code.
“In diseases classified elsewhere” codes are never permitted to be used as first-listed or principal diagnosis codes. They must be used in conjunction with an underlying condition code and they must be listed following the underlying condition. There are manifestation codes that do not have “in diseases classified elsewhere” in the title. For such codes, a “use additional code” note at the etiology code and a “code first” note at the manifestation code will still be present and the rules for sequencing apply.
Dementia with Parkinson’s Disease Example
There are different types of dementia. Dementia can be split into two broad categories -- the cortical dementias and the subcortical dementias -- based on which part of the brain is affected. Ask the provider for assistance if you are confused about aspects of the patient’s condition which can affect code assignment. “Code first” and “Use additional code” notes are also used as sequencing rules in the classification for certain codes that are not part of an etiology/manifestation combination.
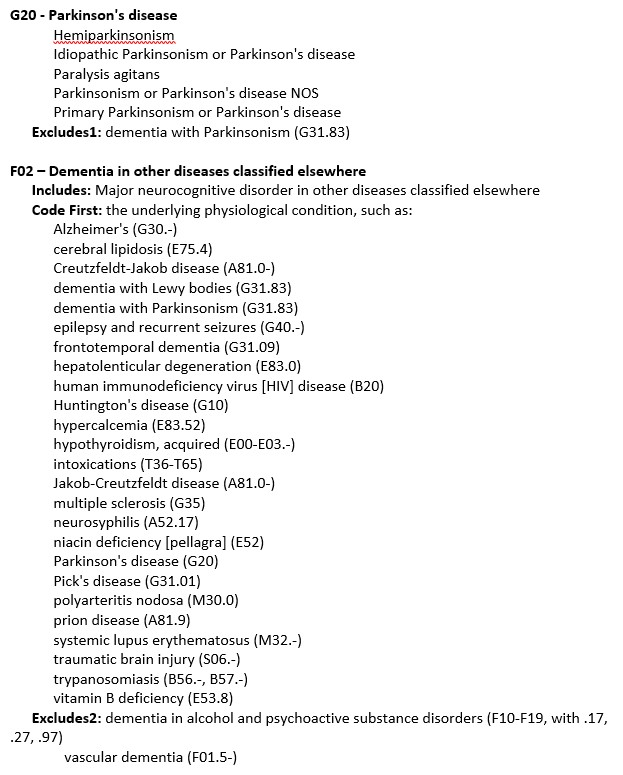
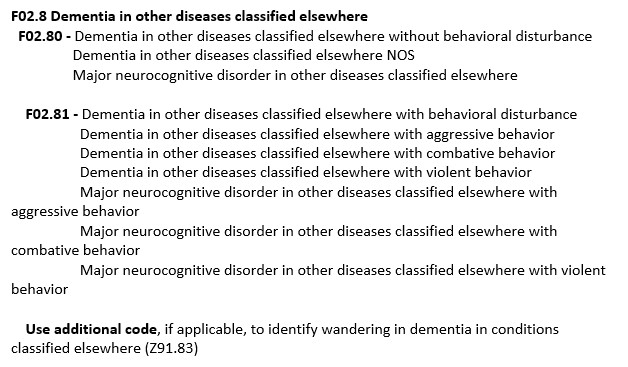
An example of manifestation coding: When coding dementia with Parkinson’s disease, reference “Dementia; with; Parkinson’s disease” in the Alpha Index. It shows G20 [F02.80]. G20 being sequenced first, followed by F02.80 on the claim form. F02.80 is the manifestation code found in brackets in the Alpha Index. If you reference Disease; Parkinson’s first, ICD-10-CM gives the code G20 but no manifestation code. You would need to then reference Dementia; with OR in (due to); Parkinson’s disease to get the G20 [F02.80]. Also verify both codes in the Tabular – here is why . . . G20 does not have a “use additional code” note but F02 has a “code first” note.
To verify G20 as the code, find G20 in the Tabular. There is an Excludes1 note but no “use additional code” note. Now reference F02.80 in the tabular, under the “F02” category we see it has a “code first” note for Parkinson’s disease (G20). Tabular listings for these codes are below to demonstrate etiology/manifestation coding and how to watch out for notes!
")
")
Acute Versus Chronic
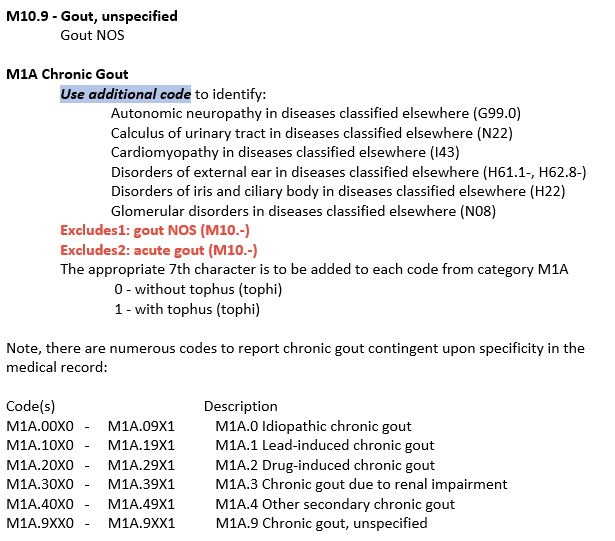
ICD-10-CM has coding conventions for when acute and chronic conditions exist. If the same condition is described as both acute (subacute) and chronic, and separate subentries exist in the Alphabetic Index at the same indentation level, code both and sequence the acute (subacute) code first. However – let’s look at an exception: Reference “Gout” in the Alpha Index. The “default” code if you have no further information is M10.9 (acute) (attack) (flare) – there is also a reference (see also Gout, Chronic).
Gout, Chronic in the Alpha Index is M1A.9. Now – let’s look both of these codes up in the Tabular. Acute & Chronic Gout: M1A.9 = “chronic gout, unspecified”, M10.9 = “gout unspecified” Gout NOS BUT – read the Excludes1 note under M1A – it excludes gout NOS (M10.-). If the patient presents with chronic gouty arthritis but the encounter is specifically for an acute flare up – what do we do?
")
The above example provides how it is essential to use both the Alphabetic Index and Tabular List when locating and assigning a code.
The Alpha Index does not always provide the full code and the guidelines are typically not provided in the Alpha Index. Selection of the full code, including laterality and any applicable 7th character, can only be done in the Tabular List. A dash (-) at the end of an Alphabetic Index entry indicates that additional characters are required. Even if a dash is not included at the Alphabetic Index entry, it is necessary to refer to the Tabular List to verify that no 7th character is required.
Sequela, Laterality and Complications of Care
A sequela is the residual effect (condition produced) after the acute phase of an illness or injury has terminated. There is no time limit on when a sequela code can be used. Coding of sequela generally requires two codes sequenced in the following order: The condition or nature of the sequela is sequenced first. The sequela code is sequenced second. Exceptions to these guidelines are those instances where the code for the sequela is followed by a manifestation code identified in the Tabular List and title, or the sequela code has been expanded (at the fourth, fifth or sixth character levels) to include the manifestation(s). The code for the acute phase of an illness or injury that led to the sequela is never used with a code for the late effect.
For lateral or bilateral sites, typically the final character of the codes in ICD-10-CM indicates laterality. An unspecified side code is also provided should the side not be identified in the medical record. If no bilateral code is provided and the condition is bilateral, assign separate codes for both the left and right side. For the second encounter for treatment after one side has previously been treated and the condition no longer exists on that side, assign the appropriate unilateral code for the side where the condition still exists.
Complications of care require specific coding based on documentation. Code assignment is based on the provider’s documentation of the relationship between the condition and the care or procedure, unless otherwise instructed by the classification. The guideline extends to any complications of care, regardless of the chapter the code is located in. It is important to note that not all conditions that occur during or following medical care or surgery are classified as complications.
There must be a cause-and-effect relationship between the care provided and the condition, and an indication in the documentation that it is a complication. Query the provider for clarification if the complication is not clearly documented.
Conclusion
Even experienced coders can use a refresh of the basics! With thoughtful preparation and development of your teaching skills, you can provide a dynamic educational environment for even the most seasoned coding professional. For more information on developing your training skills, visit our Certification Store and our Short Courses Store today!